
I never thought I would include a picture of him in my blog but what he said in his BBC interview the other day was outrageous and cruel. When challenged about the concept of “levelling up” for which Mr Gove is responsible (honestly, I don’t think even Monty Python would have thought of a Secretary of State for Levelling up), our Prime Minister responded with
‘I’ve given you the most important metric – never mind life expectancy, never mind cancer outcomes – look at wage growth. Wage growth is now being experienced faster by those on lower incomes. It hasn’t happened for 10 years or more.”
Shadow health secretary Jonathan Ashworth said the comments were “the most chilling words ever spoken by a Prime Minister.” I tend to agree. That’s many thousands of people dismissed with a toss of his fringe.
So there you are. You may have a decent wage but you may not be able to earn it because you’re riddled with what should be a preventable disease but your local hospital lacks the resources. How anyone could not realise that wage growth is a significant factor in life expectancy beggars belief but then again, nothing this Primme Minister says makes sense. It’s just uninformed waffle.
I have joined a few secondary breast cancer groups on Facebook in order to find out more about the lived experience of others. This is what I’ve learnt so far:

- Triple negative breast cancer (TNBC) is called so because it is not caused by hormones and scores zero on the Oestrogen, Progesterone and Human something Growth Receptor (HER, a protein) tests. It is a very aggressive cancer, which may explain the large number of infected lymph nodes I had in 2018 and definitely explains why I now have secondary breast cancer because it often thumbs its nose at chemotherapy. It can create lesions and tumours anywhere (OK, the eye socket is a bit weird) but most people seem to have it in their bones, liver or brain, or a combination of these. I feel fortunate but obviously, given the location which is hard to see, I’m not. We shall see. I am soooo glad I didn’t realise I had a TN tumour before now. I think I would have been permanently worried and never certain I was clear. At least ignorance gave me two years of OK-ness.
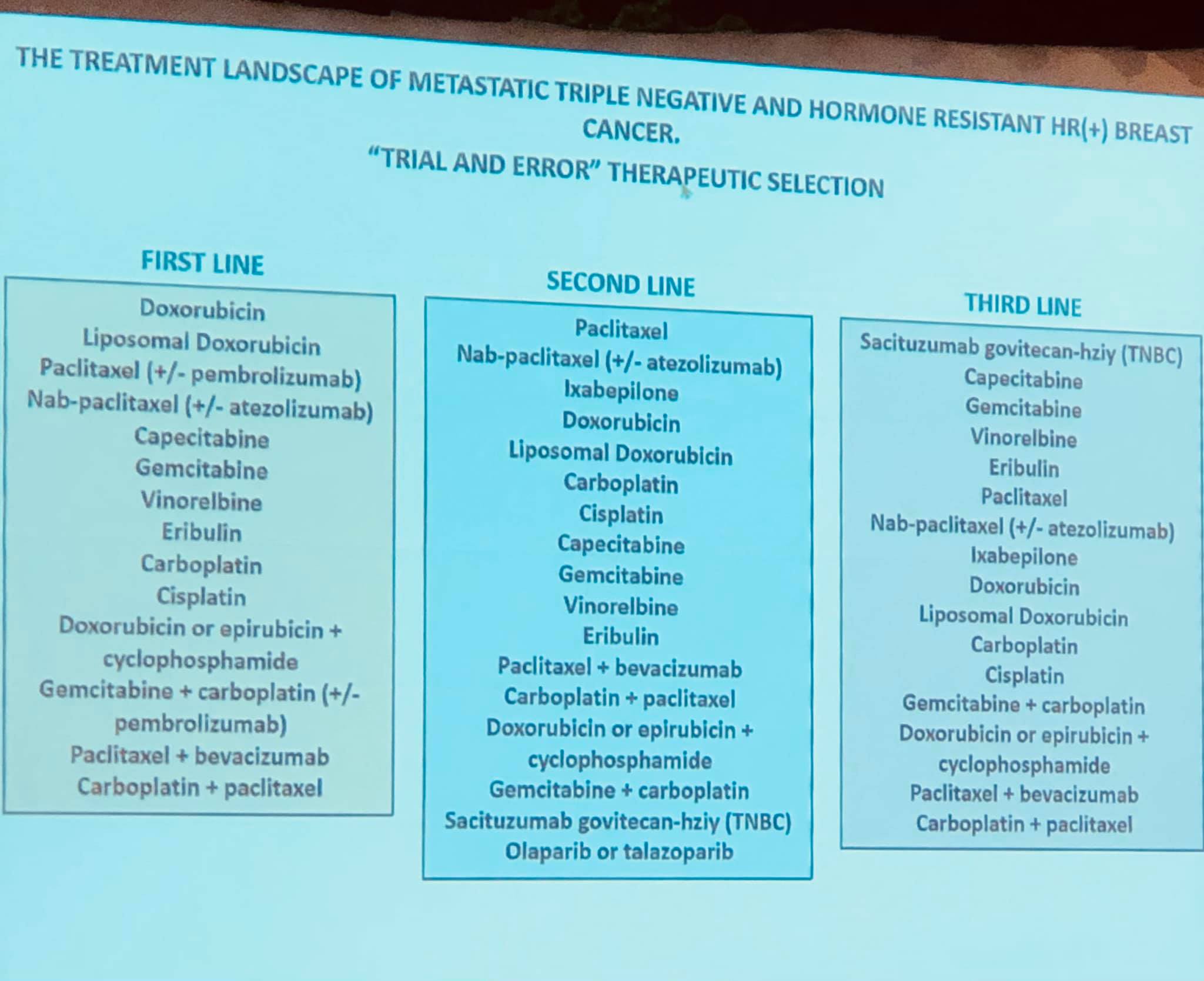
TNBC is therefore harder to treat and it seems to be guesswork and instinct that determine your treatment, whereas with a hormone receptive cancer, they obviously use treatments that work on that specific hormone. The result is that there are fewer treatment options. There seem to be plenty of drugs but there is a protocol (referred to here as the Treatment Landscape!!) that lists the drugs to be used in the first line of defence, When that fails, you are moved to the second line of defence which offers alternatives. Mine is the dreaded Paclitaxel which I had x9 first time round. Back to weekly IV and baldness. When that fails, they try the third line of defence. There is a battle going on about a new drug that is showing excellent results - it is now available to the NHS but does not have the NICE recognition yet so most hospitals maintain they can’t use it. Patients think otherwise, quite rightly, and are lobbying their MPs. They use it at St James’s but you have to have had two other failed treatments before you’re offered it. There must be sound science behind this protocol but it’s pretty scary to know it’s trial and error.
Some people last with their first drug, some get moved on within months. Touch wood, capecitabine continues to work well in controlling my cancer because I dread having 18 paclitaxel treatments. The logistics of organising lifts is terrifying in itself but maybe taxis will be safe for me by then, if I’m jabbed properly.
Some people live for years (the most I’ve seen is 22 but she now has a new spread and is most indignant). Some people die quite quickly because they don’t respond to the drugs and the spread continues. Hence Sarah Harding’s rapid decline. I fully intend being in the former group. So there.
Secondary bc is labelled incurable (pretty insensitive) because it is - once the cells have metastasised, they could be anywhere and you can feel perfectly fine and cancer-free when the buggers are settling into yet another part of your body. That doesn’t mean one is going to die, except for the fact that we all do eventually. What it seems to mean is that there is the prospect of leading a pretty shitty life of pain and sickness from the constant treatments. And the treatments and scans have to be constant because they never can tell what will happen next. That’s why they are now keeping an eye on my lung nodule and my sternum. They don’t trust the cancer to behave itself. I will be taking my 18 tablets a day for as long as capecitabine keeps my blood markers down and prevents new lesions. Oh joy!
I have also learnt that I seem to be out on a limb compared to most. Not only because of the location of my tumour (MRI results in 10 days) but because of my laissez-faire attitude. I don’t understand why I’m so phlegmatic, why I don’t get surges of anxiety (I admit to some scanxiety when it comes to results but I reckon that’s normal) and why I don’t think about dying. Maybe things will change when cape starts letting me down. I have to say when rather than if because that’s the reality - it will stop working,; we just can’t say when.
So this is a nice a cheerful post in my blog but I need to record it for my own benefit. More about vaccinations next time. What a breath-taking cliffhanger!
No comments:
Post a Comment